Why Most AI Healthcare Projects Fail After the Pilot Stage

Here is a number that should unsettle every founder and CTO building in the healthcare AI space: up to 80% of healthcare AI pilots never make it to full deployment.
The industry evidence about pilot failures shows that the process of moving from AI pilot to production is termed one of the biggest challenges in healthcare AI adoption.
They die quietly — not because the technology was wrong, not because the problem wasn’t real, but because the gap between a controlled demo environment and a living, breathing hospital system is wider than most teams anticipate.
The pilot worked beautifully. The model was accurate. The demo impressed the board. And then, somewhere between the proof-of-concept and the production rollout, the whole thing collapsed under the weight of fragmented data, resistant workflows, regulatory landmines, and costs that no one budgeted for.
This is not an isolated failure pattern. It is the rule. And understanding why it happens is the first step toward building healthcare AI applications that actually survive contact with reality.
At Tech Exactly, we have spent years working alongside healthcare founders and CTOs who hit exactly this wall. What we have learned — through 15+ HIPAA-compliant projects delivered for US digital health startups and SMBs — is that the gap between a successful pilot and a production-grade deployment is rarely a technology gap.
It is an architecture, compliance, and workflow design gap. Every failure mode covered in this blog is one we have seen up close and one we have built structured processes to prevent. The sections below break down where healthcare AI projects collapse — and hint at how the right engineering partner closes each gap before it opens.
How AI in Healthcare AI Apps Became a Noticeable Benefit
Before we diagnose the failure modes, it is worth acknowledging what genuine promise looks like — because the promise is real. Over the last five years, AI in clinical and operational settings has demonstrated measurable impact across four critical areas.
Predictive Healthcare and Early Detection
This has arguably been the most transformative application. Google DeepMind’s collaboration with Moorfields Eye Hospital produced an AI system that diagnosed over 50 eye diseases from retinal scans with accuracy matching world-leading specialists.
In oncology, AI-assisted imaging tools have demonstrated the ability to detect early-stage lung nodules that human radiologists miss on initial review.
The value proposition here is not replacing clinicians; it is ensuring that high-risk patients get flagged before conditions become catastrophic.
Personalized Patient Care
The patient care has shifted from a theoretical aspiration to a measurable reality. AI models trained on longitudinal patient data can now recommend individualized treatment protocols, predict 30-day readmission risk, and surface medication interaction flags in real time at the point of care.
Virtual Assistants and Chatbots
They have changed the front door of healthcare. Any competent AI chatbot app development company like Tech Exactly will tell you about triage bots, symptom checkers, and appointment scheduling assistants.
Operational Efficiency and Reduced Burnout
They would play a significant role in making a clear picture for you. Administrative AI tools that handle prior authorization, clinical documentation, and coding review are directly addressing the physician burnout epidemic.
It is estimated that clinicians spend nearly 50% of their time on documentation. AI that reclaims even a fraction of that time has a direct impact on provider retention and patient throughput.
The evidence of benefit is overwhelming. So why do projects keep failing after the pilot stage?
Reasons Healthcare AI Projects Collapse
Real-World Data Fragmentation: The Clean Data Trap
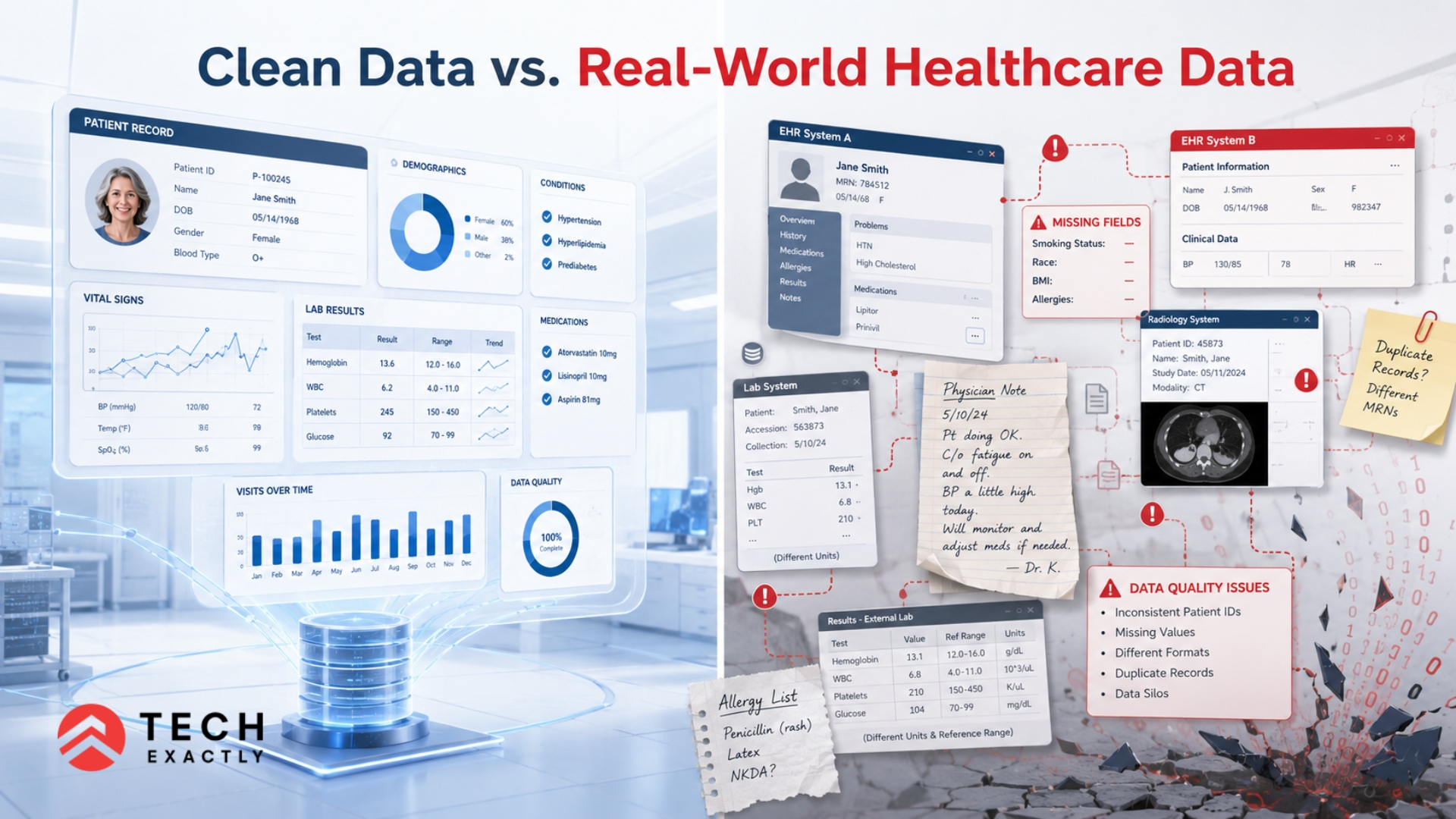
Every AI healthcare pilot is built on curated data. The real world is not curated. According to the research, several clinical AI benchmarks fail as they can’t align with the tasks of healthcare professionals, where this needs to be automated. Further, creating a gap between the project success and production value.
Curated vs. Chaotic Data
During the pilot phase, data scientists work with carefully selected, labeled, and cleaned datasets. The model trains well, validation metrics look strong, and everyone believes the system is production-ready.
Then it hits the actual EHR data — and the model encounters inconsistent date formats, missing lab values coded as zero instead of null, provider notes written in idiosyncratic shorthand, and demographic fields populated with placeholder values.
The performance cliff is immediate and severe. Any skilled mobile app developer building in this space will confirm that data preprocessing alone can consume 60 to 80 percent of engineering time in production environments.
System Silos
Healthcare data is fractured across incompatible systems. A single patient’s journey may span a primary care EMR, a separate radiology PACS, a pharmacy management platform, and a billing system — none of which speak the same data language.
HL7 FHIR has improved interoperability in theory, but implementation quality varies wildly across vendors and hospital IT departments.
Aggregating a coherent patient record for real-time inference is a significant engineering challenge that pilot environments typically sidestep entirely.
High Failure Metric
IBM Watson for Oncology is the cautionary tale the industry cannot stop citing. After years of development and deployment at major cancer centers, the system recommended treatments that oncologists at MD Anderson and Memorial Sloan Kettering described as unsafe and incorrect.
The root cause traced back to training data that did not reflect the actual diversity and complexity of real patient populations. The failure was not a product failure — it was a data representatives failure that the pilot stage never surfaced.
One of the most discussed examples of AI deployment challenges in healthcare is IBM Watson for Oncology. This plays a significant role in emerging concerns around recommendation quality and training methodology.
Workflow Friction and Cognitive Load
Building a model that works is different from building a product that gets used.
The Two-Click Rule
Clinical staff operate under extreme time pressure. In a typical primary care visit, a physician has 15 to 20 minutes with a patient. If an AI recommendation requires more than two clicks to access, interpret, and act on, it will be ignored.
Every unnecessary step in the UX is a reason for adoption to fail. This is where working with an experienced mobile app development company that understands clinical workflow design makes the difference between a tool that clinicians champion and one they route around.
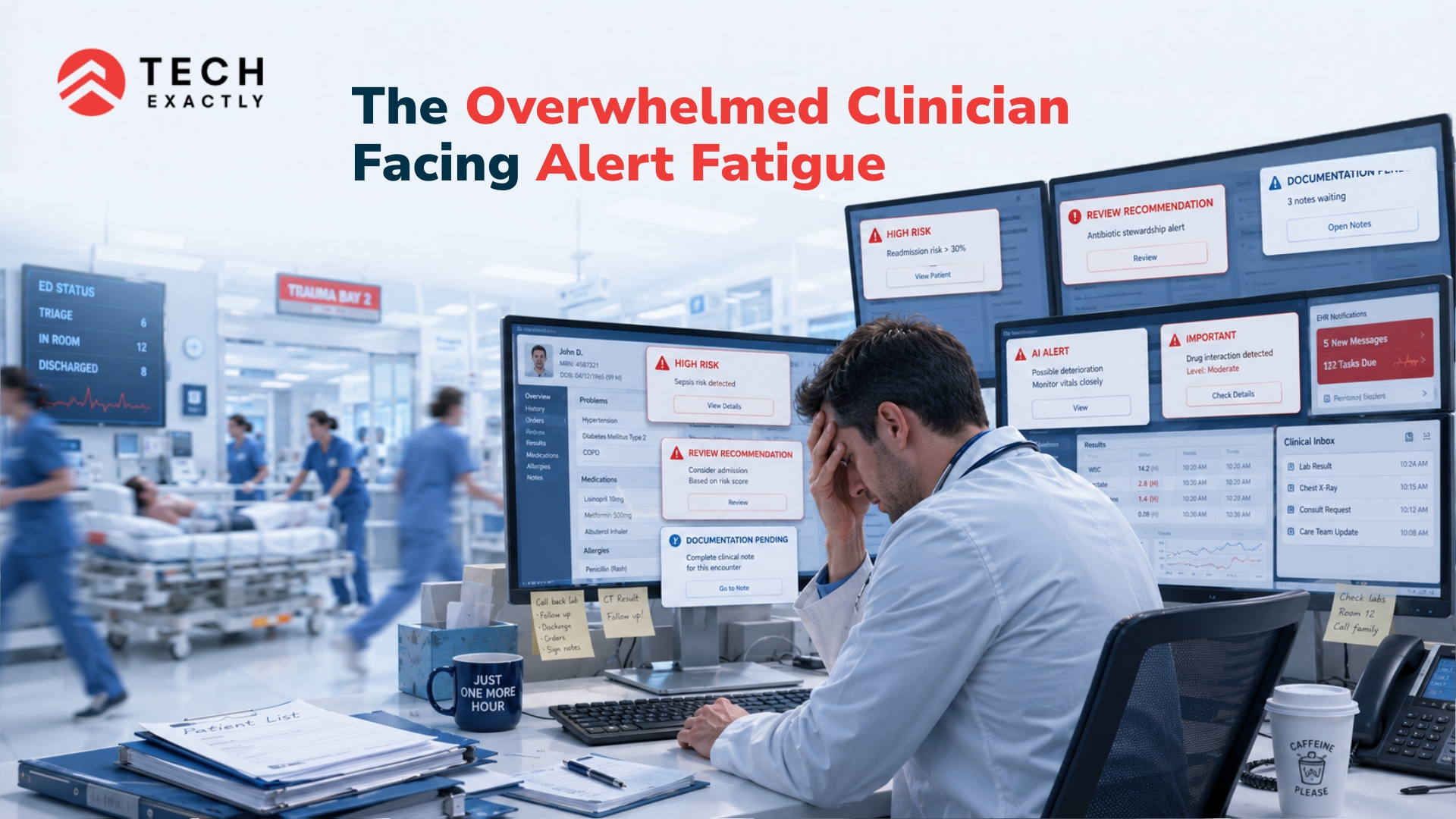
Alert Fatigue
Healthcare AI systems have a dangerous tendency to over-alert. When a system flags everything as high-priority, clinicians learn to dismiss everything.
Studies on sepsis prediction tools in ICU settings have found that even high-accuracy models get ignored when alert specificity is low — because staff are already managing 30 to 50 alerts per shift from existing monitoring systems. The AI adds noise, not signal, and adoption craters.
The teams that consistently succeed are those that hire a skilled mobile app developer with React and treat product design as a first-class discipline, not an afterthought.
Capability vs. Product Optimization
Many healthcare AI teams are staffed with exceptional data scientists and clinicians but lack the product engineering depth to translate model capability into clinical usability. Building a model with 94% AUC does not automatically translate into a product that integrates cleanly into a physician’s morning workflow.
The teams that consistently succeed are those that treat product design as a first-class discipline, not an afterthought. Following mobile app development tips tailored for regulated, high-stakes environments — like shadow mode deployment, phased rollout with feedback loops, and in-situ user testing — separates successful deployments from shelved pilots.
Technical and Integration Complexity
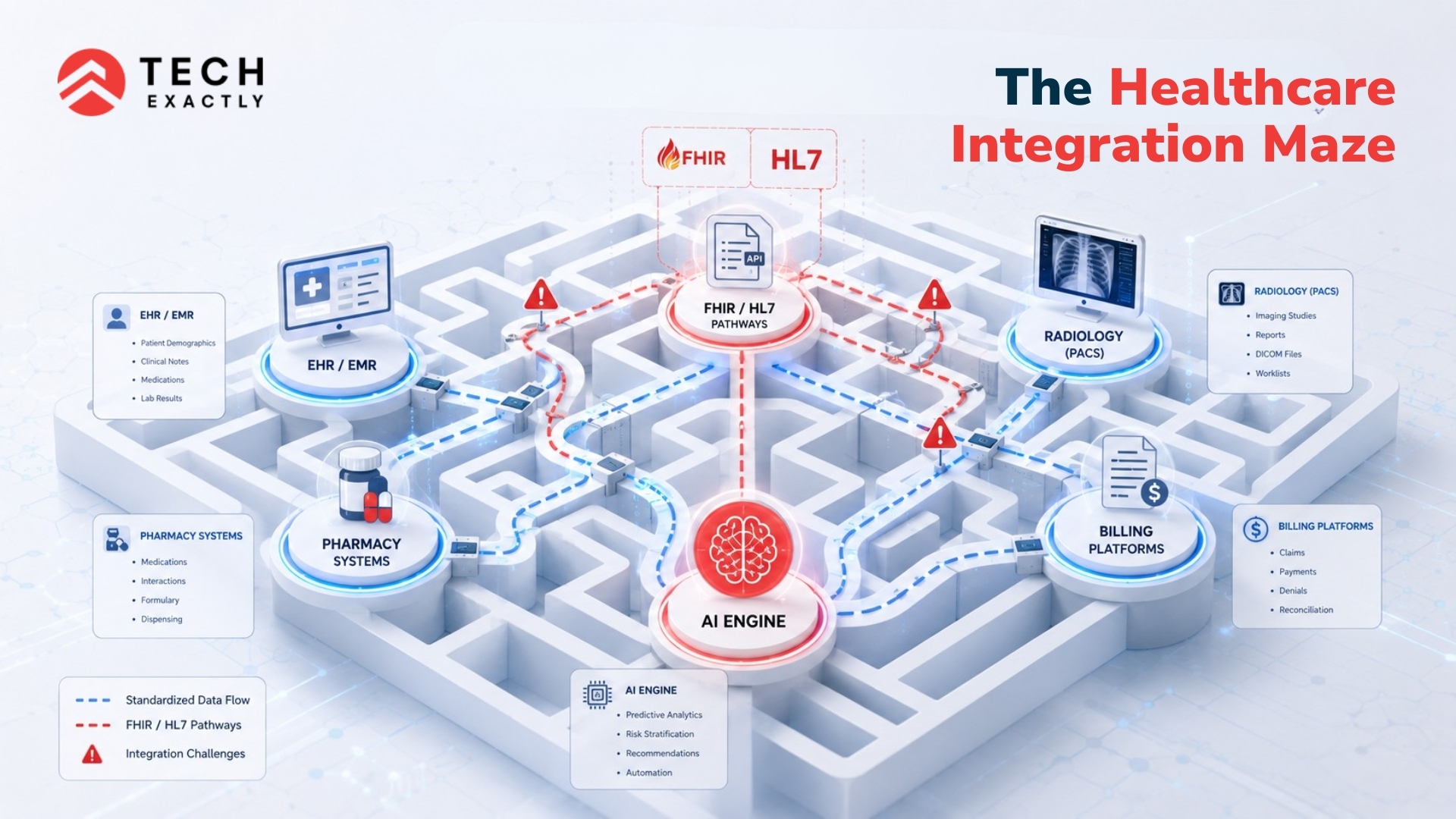
EHR Integration Obstacles
Epic and Cerner collectively control a significant share of the hospital EHR market. Both offer integration pathways, but the reality of implementing against their APIs in a production enterprise environment is significantly more complex than development sandboxes suggest.
Credentialing requirements, data access governance, and the sheer variability of how different health systems configure their EHR instances mean that integration work that took two weeks in the pilot can take six months in production. Any AI App Development Company in the USA operating in this space without deep experience in EHR integration will encounter this wall.
Lack of MLOps
Pilot models are static snapshots. Production clinical AI requires continuous monitoring, retraining pipelines, drift detection, and version governance.
A sepsis prediction model trained on pre-pandemic ICU data performs very differently on a post-pandemic patient population with altered comorbidity profiles.
Without a mature MLOps infrastructure — model registries, automated retraining triggers, performance dashboards, rollback protocols — the model degrades silently. No one notices until outcomes data starts looking wrong.
Delayed Governance and Regulatory Friction
Late Compliance Checks
The FDA’s Software as a Medical Device (SaMD) framework, HIPAA technical safeguards, and state-level data privacy regulations are not features to be added at the end of the development cycle. They are architectural constraints that must be built in from the first sprint.
Teams that treat compliance as a final gate — rather than an ongoing design consideration — discover in late-stage deployment that their data handling architecture, consent framework, or model explainability documentation do not meet regulatory requirements. The rework cost at that stage is catastrophic.
Security Bottlenecks
Healthcare organizations have among the most rigorous security review processes of any industry — and for good reason. A healthcare data breach costs an average of $10.9 million per incident, the highest of any sector.
The security review cycle for a new AI system touching PHI can take three to nine months at large health systems. Teams that do not plan for this in their go-live timeline routinely find their production launch delayed by a full year.
Accountability Gaps
When an AI-assisted diagnosis contributes to an adverse patient outcome, the question of accountability is immediate and legally consequential.
Most healthcare organizations will not deploy AI systems — regardless of accuracy — without a clearly defined accountability framework: which recommendations require physician override, how the model’s reasoning is documented in the clinical record, and what the escalation protocol is when the system’s confidence is below a defined threshold. Pilots that skip this design work cannot clear the deployment approval process at any risk-averse institution.
The Financial Chasm
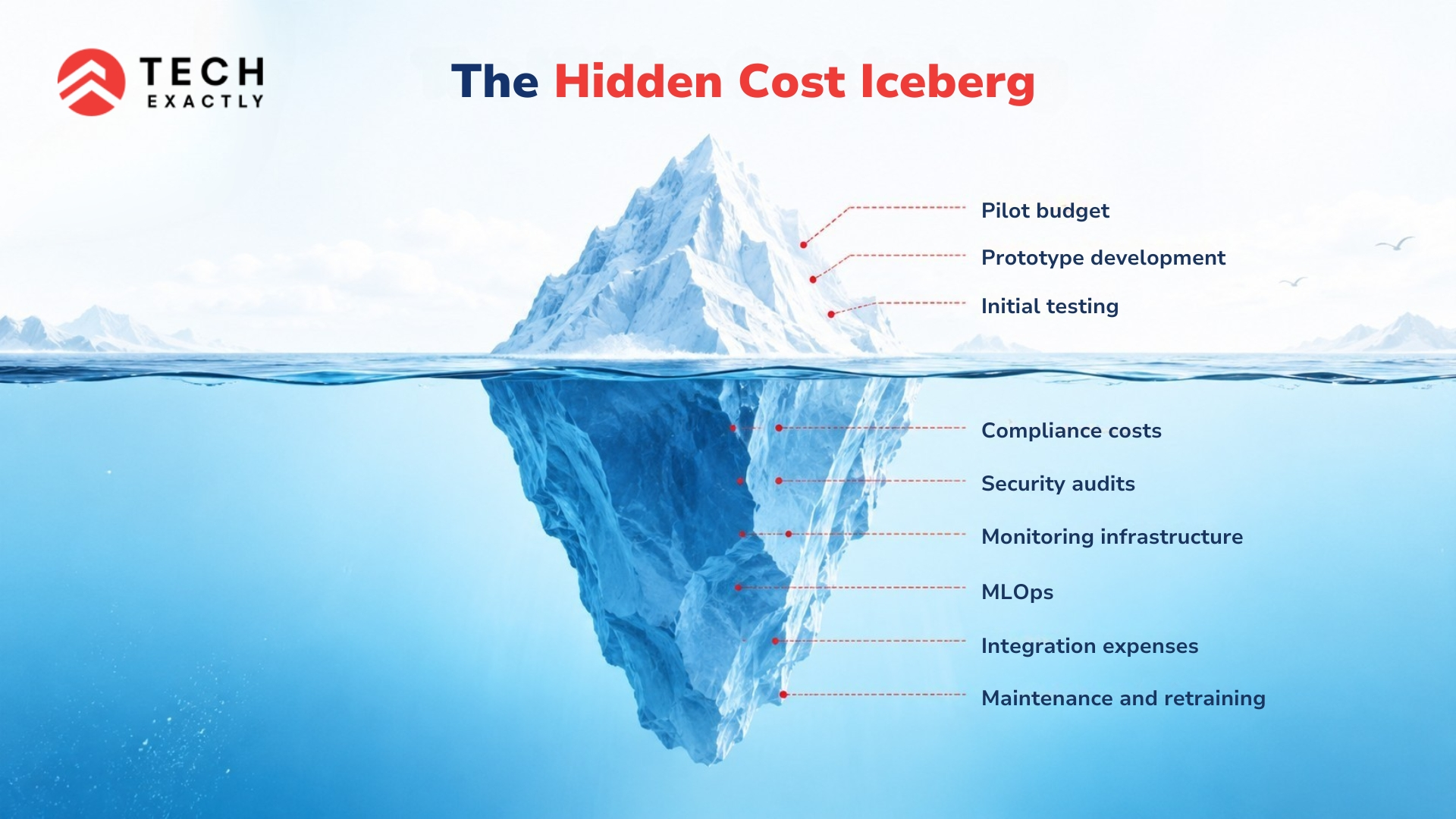
Hidden Scaling Costs
Pilot economics is flattering and misleading. Running inference on a few thousand patient records in a controlled environment bears almost no resemblance to the infrastructure cost of serving predictions at scale across a multi-hospital system.
Data storage, compute, API calls, monitoring tools, and compliance infrastructure combine to create a cost structure that consistently surprises founding teams. The gap between “pilot budget” and “production operating cost” has ended more than a few otherwise viable companies.
Funding Dry Spells
The pilot-to-production transition typically requires a 12 to 24-month runway of sustained investment before a healthcare AI product generates meaningful revenue.
Reimbursement pathways are slow to develop, health system procurement cycles are long, and value-based contracting models that tie payment to outcomes are still maturing.
Companies that raise enough to build and pilot a product but underestimate the capital required to survive the deployment and commercialization phase run out of runway in the gap.
An experienced AI-powered mobile app development company with depth in the healthcare sector will model this financial transition explicitly before committing to a go-live timeline.
Final Thoughts
The AI healthcare pilot problem is not a technology problem. The models are good enough. The clinical use cases are validated. The failure is almost always an execution and systems design problem — fragmented data architectures, misaligned workflows, incomplete regulatory preparation, and financial models that do not account for the true cost of production deployment.
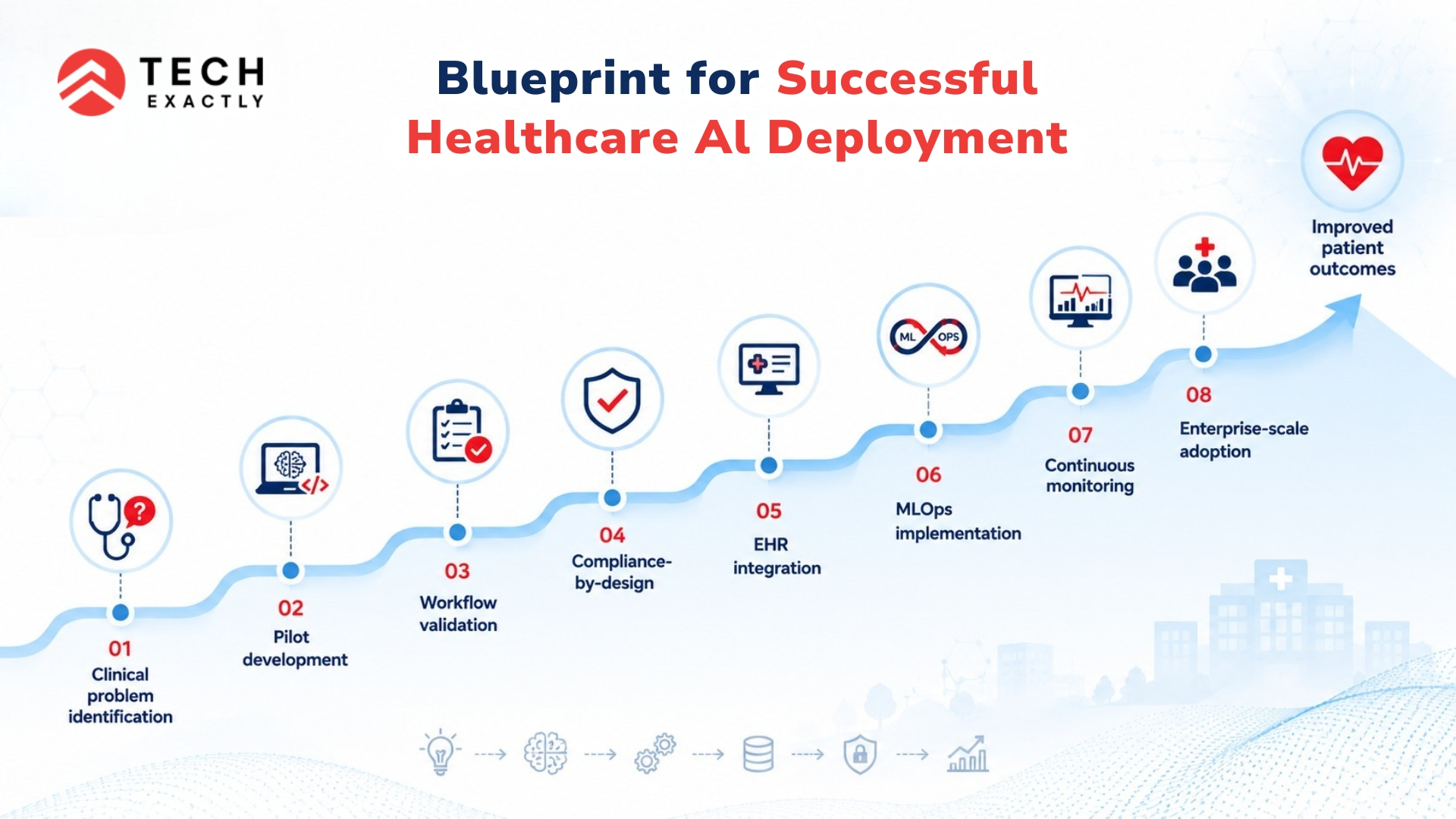
The teams that make it through — that build healthcare AI products that stick, scale, and genuinely improve patient outcomes — are the ones that treat the pilot not as proof of technology but as a stress test of every assumption that production will challenge.
They instrument their pilots for real-world data heterogeneity. They co-design workflows with frontline clinicians. They build compliance in from sprint one. They model production economics honestly.
If you are a founder or CTO navigating this transition, the difference between a shelved pilot and a deployed product often comes down to the partners you build with and the architecture decisions you make in the first 90 days.
Building healthcare AI that survives the pilot stage requires the right technical foundation and the right team. Discussing the AI approach around the product architecture for regulated clinical environments can be a way to go.
Among all, the team at Tech Exactly can minimise technology gaps and deliver a seamless AI healthcare project.

